



Providing information about both the health hazards of cooking with solid fuel and subsidy benefits led to behavioural changes and increased LPG usage
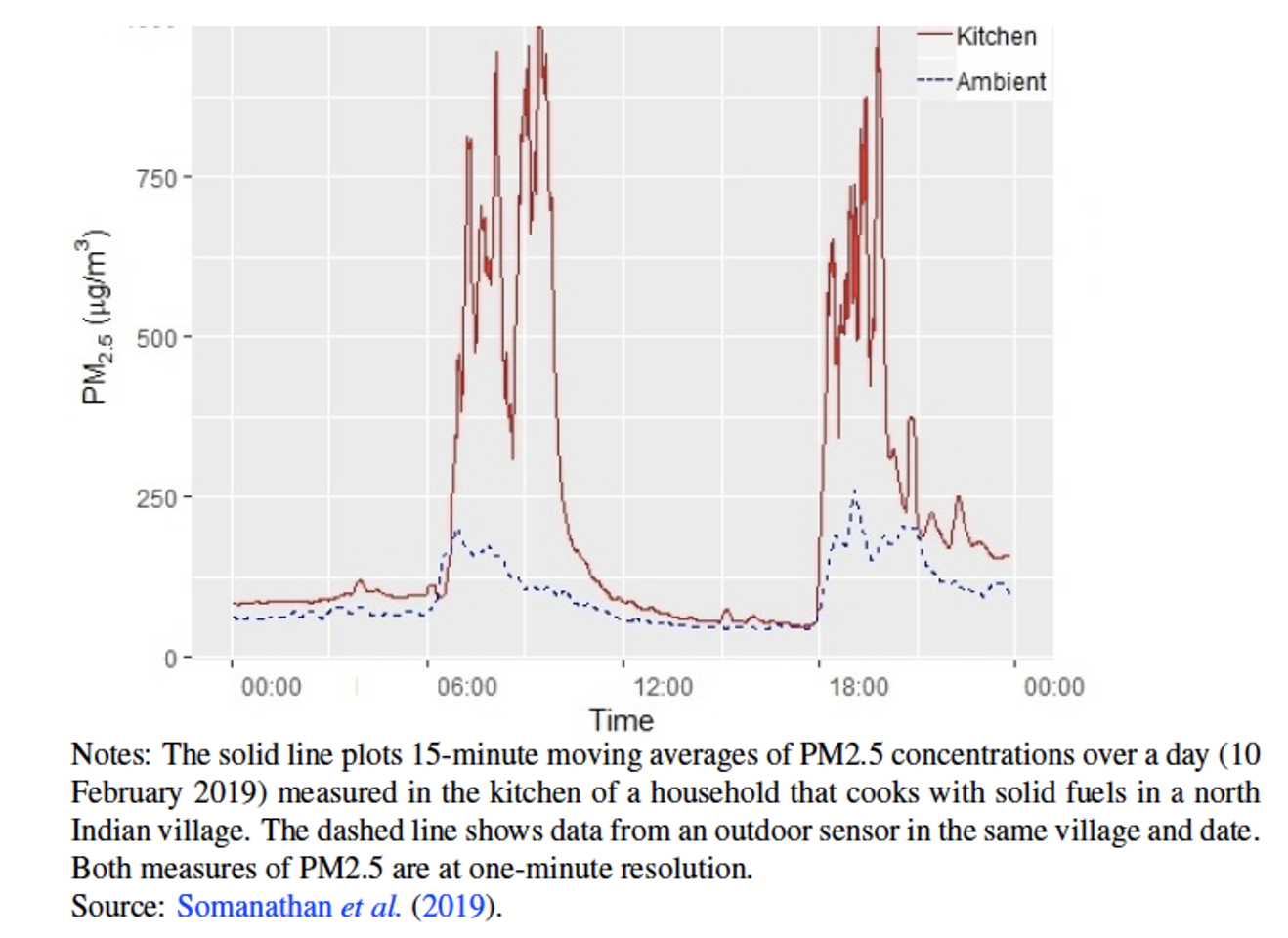
In a ranking of the world's most polluted cities by IQAir, more than 20 of the world's 30 most air-polluted cities are in India. Household sources are the single largest contributor to ambient air pollution in much of the developing world, including India. Air pollution levels within households that cook with solid fuels such as wood and cow dung can be high and skyrocket to 40 times greater than the safe limit prescribed by the WHO (see Figure 1).
Figure 1 Air pollution levels within households that cook with solid fuels
Bottled liquid petroleum gas, or LPG, is the most commonly used clean cooking fuel in Asia and Africa (see Figure 2). However, financial constraints are a major reason for poor households not switching entirely to LPG. Even when LPG usage is subsidised, the cost can remain considerable for poor households. There is little awareness of the long-term health hazards of cooking with solid fuel. These include pre-term deaths and low birth weight of infants born to mothers who inhale smoke from solid fuels during pregnancy, as well as respiratory, cardiovascular and eye diseases. WHO estimates that 3.8 million premature deaths were attributable to household air pollution in 2016 in low- and middle-income countries.
Figure 2 Illustration of LPG Cylinder and cooker
In order to expand LPG access particularly to disadvantaged households, the Government of India launched its flagship programme, Pradhan Mantri Ujjwala Yojana, in April 2016. The Ujjwala scheme is the largest programme on access to clean fuel in India’s history and in the world, reaching 72 million poor families by June 2019. But, the average annual usage of LPG by existing and newly connected rural households remains less than half of what is needed to eliminate solid fuel use.
In assessing LPG coverage and use, we conducted a survey of 3,000 rural households in 150 villages of Indore district (in the state of Madhya Pradesh) in 2018. Only 65% of households in our survey had an LPG account despite of the Ujjwala program. Annual refill consumption was approximately 4.5 cylinders in households with LPG connection (across both Ujjwala eligible households and non-Ujjwala households) even though the government subsidises up to 12 refill purchases per year. Our survey also revealed that 87% of the sampled households were unaware of the serious long-term risks to their health. In addition, 33% of sampled households with LPG accounts disagreed that the government deposits a subsidy in their bank account after they purchase an LPG cylinder and only 51% agreed that their out-of-pocket expenditure was less than the market price of an LPG refill.
The LPG subsidy was universal until 2021, with the government targeting a fixed subsidy of 200 rupees per LPG cylinder to only Ujjawala programme beneficiaries in 2022. However, 32% of respondents believed that the refill subsidy was not universal and only Ujjawala customers were eligible to receive the subsidy. This is not surprising, given the complex cash-back design of the subsidy programme. Under the subsidy scheme, a consumer with an LPG account would buy an LPG cylinder refill at the market price and then receive a transfer of the subsidy amount to their bank account about 2–3 days after the purchase. In addition, the market price of a cylinder refill varied significantly (between 654 and 879 rupees during November 2017 to October 2018) in tandem with the international price of LPG, keeping the post subsidy price stable at around 500 rupees.
Following our 2018 household survey, we designed and implemented a cluster-randomised controlled trial in the 150 sampled villages in 2019, to improve awareness about the health hazards of cooking with solid fuels and subsidy benefits with the objective of increasing regular LPG use (Afridi et al. 2021). The intervention had two treatment arms: in the first, awareness about the adverse health effects of cooking with solid fuels was provided to household members (H); in the second, the existing cashback payments from the government after purchasing a refill of LPG at market price (H+S) were explained in addition to health awareness. The control group of villages were provided no information. Each arm consisted of 50 sampled villages and 1,000 households therein.
Besides partnering with India’s Ministry of Petroleum and Natural Gas and the three public sector oil marketing companies (OMCs) for access to LPG consumer level data, we embedded our awareness campaign within the rural public health system. Existing frontline public health workers (Accredited Social Health Activists, or ASHAs) in the villages were trained to conduct a door-to-door campaigns by making up to 6 household visits over a nine-month intervention period starting in January 2019 in the 100 treatment villages. These workers were incentivised financially in a manner and at a rate comparable to their existing remuneration.

Photo of ASHA worker in purple with treatment household
Using OMCs’ LPG consumer-level refill consumption data, we compared the annual and monthly LPG consumption by the households in our sample before and after the intervention, and relative to the control group. We find that our intervention led to an insignificant increase in annual LPG refill consumption. However, in the combined (H+S) treatment arm, households with a head who had completed less than primary schooling increased annual refill consumption significantly by 10-12%, compared to those whose head was primary educated (or more). These households are also more likely to be the ones that need to be informed about the health hazards of indoor air pollution and the implications of the cash-back subsidy.
We analysed LPG consumption at monthly (rather than annual) frequency, controlling for seasonality in fuel usage and internationally determined LPG refill prices. We also allowed for unobserved heterogeneity across sub-districts and found that there was an 8.6% increase in refill consumption due to the overall treatment. This result was driven by a 12.5% rise in monthly refill consumption in the combined (H+S) treatment. Furthermore, the usage of electric or induction stoves for cooking increased significantly by 45–50% and 58–63% from the baseline average usage of 6% in the overall and combined treatment arms, respectively. This suggests that there was substitution towards a clean fuel which is relatively cheaper than LPG.
Although health information alone did not increase consumption of LPG refills (annually or monthly), it led to significant behavioural changes that could reduce the inhalation of indoor smoke. H treatment group of households were 5 percentage points more likely to have an outlet for smoke from traditional stoves (also due to treatment overall and in combined arm) and/or use a separate room as a kitchen (also overall treatment), compared to the control group that did not receive any information. The probability that households used only traditional cooking stoves to prepare the last meal decreased marginally by 5 percentage points in the health information-only treatment. There was an insignificant decline in firewood or dung use (extensive margin measure) in the preceding month, but the usage of clean fuels in preparing the last meal (intensive margin measure) rose in all treatment arms.
This is the first study to measure the extent to which awareness impacts mitigating behaviour in the case of air pollution. Our findings have implications for clean fuel adoption well beyond India's LPG programme as several developing countries expand their electricity networks, bringing the possibility of electric cooking with induction stoves to hundreds of millions of people. The small effect sizes on LPG usage underline the limited impact of increasing awareness and the salience of the financial constraints that households face in using LPG regularly for cooking instead of wood and cow dung. These sources of cooking fuel which are often freely available while the cost of one LPG cylinder refill (at market price and before subsidy cash-back) can vary anywhere between US$8–12. This is a substantive cost for households with average monthly income of $100.
From a policy perspective, our results indicate complementarity between improving health awareness and loosening financial constraints. Poor households may not transition to regular usage of clean fuels even if they are aware of the long-term damage caused to their health by indoor air pollution. More specifically, our findings underline the importance of public subsidy design for clean fuels, both in terms of comprehension and timing. Households that were able to comprehend the cash-back nature of the LPG subsidy internalised the information that their out-of-pocket expenditure is lower than the market price they pay upfront. More importantly, depositing the subsidy amount upfront into the accounts of beneficiary households could substantively reduce the financial burden on liquidity and credit-constrained households and increase LPG take-up further.
References
Afridi, F, S Debnath and E Somanathan (2021), “A Breath of Fresh Air: Raising Awareness for Clean Fuel Adoption”, Journal of Development Economics, 151: 102674.