




Women have a stronger preference for contraceptive vouchers than their spouses in monogamous households, but a weaker preference in polygynous ones
In recent decades, fertility has decreased substantially in most developing countries, with the exception of sub-Saharan Africa where it remains high (United Nations 2019). Despite the increased availability of modern contraceptives, less than 25% of women in sub-Saharan Africa use them (United Nations 2017). Could this be due to the high prevalence of polygyny? 25% of married women in sub-Saharan Africa live in polygynous households (Arthi and Fenske, 2018), and in West-Africa almost 40% (Dalton and Leung, 2014).
A large literature has looked at the link between polygyny and fertility. Two opposing effects of polygyny on fertility have been suggested. First, women in polygynous households might face greater pressure to become pregnant than monogamous women, since polygynous households’ co-wives might compete with one another around fertility. Having more children might increase social status and access to household resources (Jankowiak et al. 2005, Bove and Valeggia 2009, Lambert and Rossi 2016, Mammen 2019). We call this a ‘competition effect’. Second, husbands in polygynous households may divide their ideal number of children between co-wives (Pebley et al. 1988, Pison 1986). This would reduce men’s pressure on women’s fertility through a so-called ‘substitution effect’, so that women’s fertility might actually be lower in polygynous households than in monogamous households.
Varying the husband’s involvement
The first effect influences women's preferences while the second effect influences men's preferences. To separate both effects, in our study (D’Exelle, Lépine, Bakyono, and Tapsoba 2021), we experimentally vary the influence of men and women in the decision-making process amongst monogamous and polygynous households. To do this, we carried out a randomised controlled trial with 1,074 monogamous and polygynous couples in rural Burkina Faso, who did not use contraceptives. In the experiment, we gave couples a voucher that provides women access to a free modern contraceptive of their choice, supplied by local health facilities. We varied the husband's involvement in the decision-making process by randomising whether the voucher is given to women alone (‘woman treatment’) or to the husband with their wife being present (‘couple treatment’). The voucher could only be used by the couple who received it. The voucher was given at the end of a private interview with the woman, to collect information on aspects such as fertility preferences, extent of friendship with co-wives (a simple yes/no question whether they were friends with co-wives), co-wife rank (which corresponds to who got married first, second, etc. with the husband).
As can be observed in Figure 1, involving the husband lowers contraceptive use amongst monogamous women but increases its use amongst polygynous women who face co-wife rivalry, as proxied by a lack of co-wife friendship. We also find that this is driven by lower-ranked co-wives. We do not find any effect amongst polygynous couples where there is no co-wife rivalry. This suggests that monogamous women have a stronger preference for contraceptives than their respective husbands, while this difference in preferences is smaller or even reversed amongst polygynous households. The latter could be driven by co-wife competition and the husband’s preference to use contraception where there is co-wife rivalry.
Figure 1 Treatment effects on average use of contraceptives
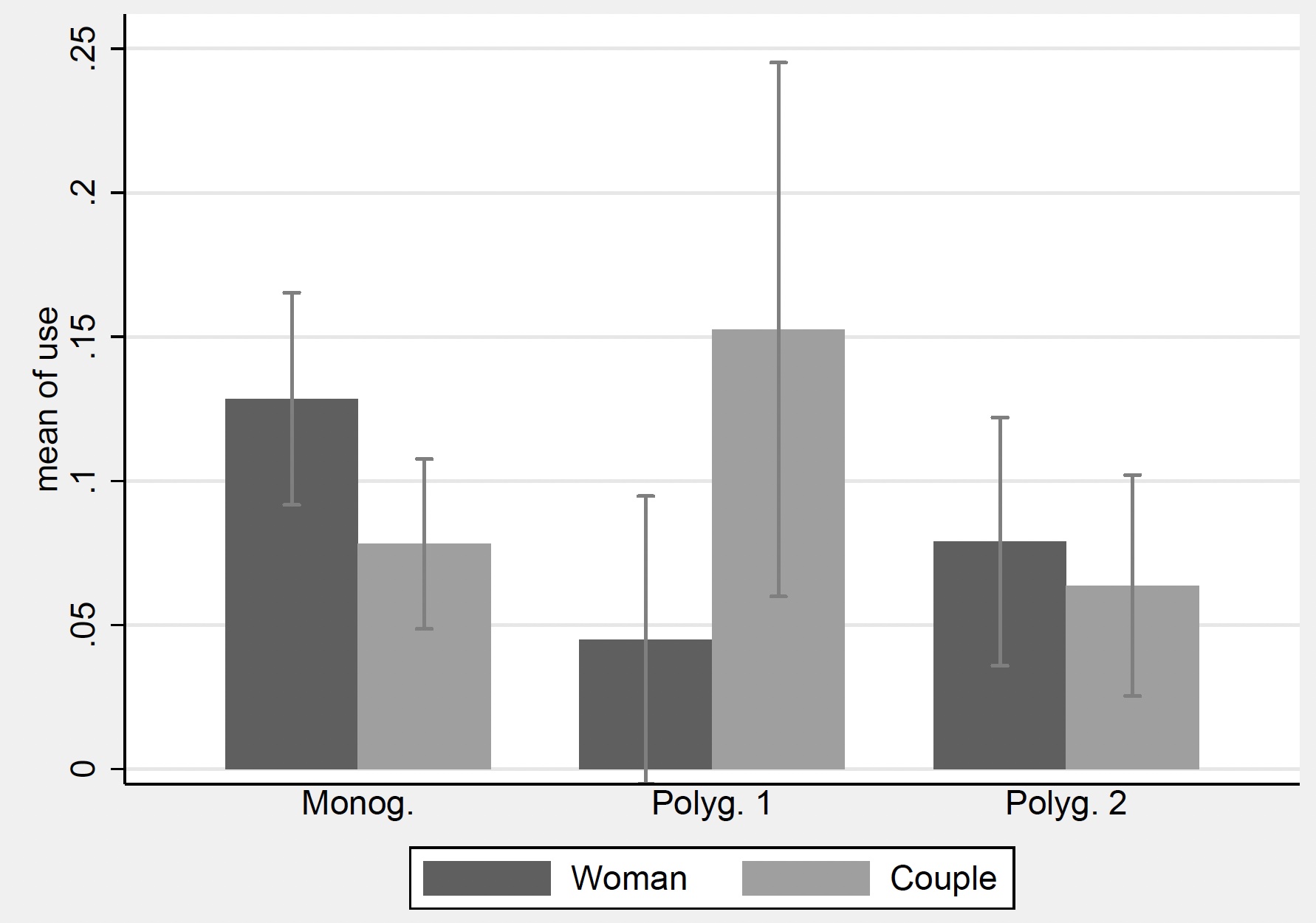
Note: Polyg. 1 = polygynous couples where there is co-wife rivalry; polyg. 2 = polygynous couples without co-wife rivalry. Couple = couple treatment. Woman = woman treatment. 95% confidence intervals used.
Competition versus substitution
To disentangle the competition and substitution effects, we compare voucher use within each treatment. In Figure 2, we observe that in the woman treatment, voucher use is lower amongst polygynous women than amongst monogamous women. Furthermore, voucher use is lowest amongst polygynous women who face co-wife rivalry. Additional analysis indicates that this is again driven by co-wives of lower rank, and it is stronger where the first wife has more children. This evidence provides strong support for a competition effect.
In the couple treatment, voucher use is lower amongst polygynous households than amongst monogamous households, but again only when we focus on second wives who are not friends with co-wives. This is not consistent with a substitution effect. If the difference in voucher use was the result of a substitution effect, it should not depend on co-wife friendship or rank. This suggests that something else is driving this result. We see two possible explanations:
- Husbands in polygynous households are under pressure to maintain harmony in the household. As competition around fertility affects co-wife friendship and the spousal relation, husbands can try to reduce tensions amongst co-wives with contraception.
- It is possible that husbands might care less about lower-ranked wives, possibly influenced by the first wife where there is no co-wife friendship. As a result, husbands would be less inclined to support the fertility preferences of co-wives of lower rank.
Figure 2 Average use of contraceptives by polygyny status
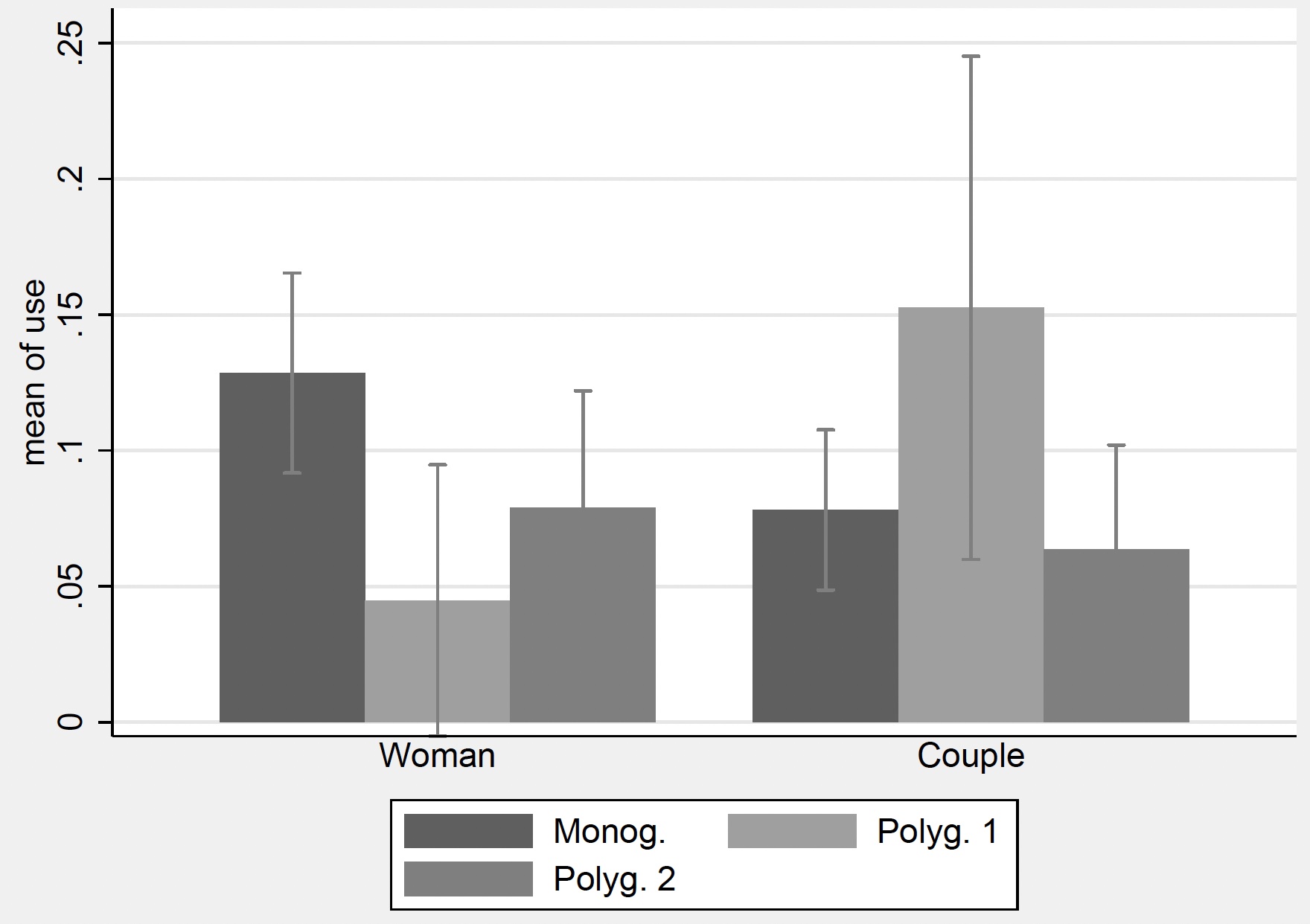
Note: Polyg. 1 = polygynous couples where there is co-wife rivalry; 2 = polygynous couples without co-wife rivalry. Couple = couple treatment. Woman = woman treatment. 95% confidence intervals used.
Effectiveness of the intervention
Further analysis shows that most effects are driven by women who used modern contraceptives before, and therefore stopped using them (none of the women in the sample used contraceptives when they were recruited into the experiment). This is an important finding, as the continuity of contraceptive use is important for the effectiveness of contraception and a large proportion of women in our sample had stopped using contraceptives. Most of these women did so as they wanted to have another child (55.81%), or because of side effects of contraceptives (18.68%).
Looking at the type of contraceptives chosen, we find that the use of the voucher translates mostly into the use of long-term contraceptives, such as implants, rather than injectables, which give more short-term protection (up to three months).
While we found important treatment effects on voucher use and the choice of contraceptives, it is important to test whether they translate into differences in pregnancy rates and
contraceptive use after the experiment. To test this, we interviewed all participants again six months after the experiment. We find that the use of the voucher increases the likelihood of contraceptive use by more than 50 percentage points and decreases the probability of pregnancy by 13-15 percentage points.
Policy implications
The following policy insights are supported by our findings.
- Family planning services offered by health centers increases contraceptive use and reduces pregnancy rates. Their use, however, is low, which remains an important challenge.
- The involvement of the husband has opposing effects on contraceptive use amongst monogamous and polygynous households. This insight can be exploited by policymakers. Specifically, the uptake of contraceptives in monogamous households could be increased by either bypassing husbands or by aiming to reduce men's fertility preferences, while in polygynous households with co-wife rivalry, contraceptive use could be increased by involving the husband, or by weakening co-wife rivalry around fertility.
- The involvement (or not) of the husband would be most effective for the use of long-term contraception, and for couples who stopped using contraceptives.
- As we found strong evidence for a competition effect, but also evidence that when the husband is involved (couple treatment), polygyny increases contraceptive use where there is co-wife rivalry, we cannot draw any conclusions about the contribution of polygyny to the high fertility rates in sub-Saharan Africa.
References
Arthi, V and J Fenske (2018), “Polygamy and Child Mortality: Historical and Modern Evidence from Nigeria's Igbo", Review of Economics of the Household 16: 97-141.
Bove, R and C Valeggia (2009), “Polygyny and Women's Health in sub-Saharan Africa”, Social Science and Medicine 68(1): 21-29.
Dalton, J T and T C Leung (2014), “Why Is Polygyny More Prevalent in Western Africa? An African Slave Trade Perspective”. Economic Development and Cultural Change 62(4): 599-632.
D’Exelle, B, A Lépine, R Bakyono and L Tapsoba (2021), “Fertility and Polygyny: Experimental Evidence from Burkina Faso”, Working Paper.
Jankowiak, WR, M Sudakov and BC Wilreker (2005), “Co-wife Conflict and Cooperation”, Ethnology 44: 81-98.
Lambert, S and P Rossi (2016), “Sons as Widowhood Insurance: Evidence from Senegal", Journal of Development Economics 120: 113-127.
Mammen, K (2019), “All For One Or Each For Her Own: Do Polygamous Families Share and Share Alike?", Journal for the Advancement of Developing Economies 8: 39-55.
Pebley, A, W Mbugua and N Goldman (1988), “Polygyny and Fertility in Sub-Saharan Africa", Fertility Determinants Research Notes 21: 6-10.
Pison, G (1986), “La Démographie de la Polygamie”, Population (French Edition) 41(1): 93-122.
United Nations (2017), World Family Planning 2017: Highlights, United Nations, Department of Economic and Social Affairs, Population Division.
United Nations (2019), World Population Prospects 2019: Highlights, United Nations, Department of Economic and Social Affairs, Population Division.