

Gender gaps in child health have narrowed in India, but important gaps remain both for girls and younger brothers, and sex-selective abortion poses a new challenge
Thirty years ago, Amartya Sen called attention to the 37 million “missing women” in India. They were part of the more than 100 million girls and women worldwide who would have been alive but for gender discrimination (Sen 1990, 1992). At that time, gender discrimination took the form of infanticide or inadequate nutrition and health care for girls and women. The problem has since changed in nature, both for better and worse. The gender gap in child survival has narrowed, but now there are millions of girls missing because they were never even born. The advent of prenatal sex determination technology has enabled couples who want a son, not a daughter, to selectively abort female fetuses.
In my research (Jayachandran 2023), I provide an overview of son preference in India – its current state and recent trends - discussing both parents’ favouritism toward sons when providing inputs such as healthcare and their desire to give birth to sons. This article is organised around ten facts.
Gender gaps in health
Facts 1 to 3: Gender gaps in child health inputs and outcomes have narrowed in recent decades. However, important gaps remain, and policies beyond free health services are needed to close them.
Using the five waves of India’s National Family Health Survey (NFHS), conducted from 1992-3 to 2019-21, I show that the gender gap in vaccinations has closed over the past thirty years, as shown in Figure 1. Similarly, India’s excess female mortality of infants has declined in recent years.
Figure 1: Female-male ratio of vaccinations in India across waves of the National Family Health Survey
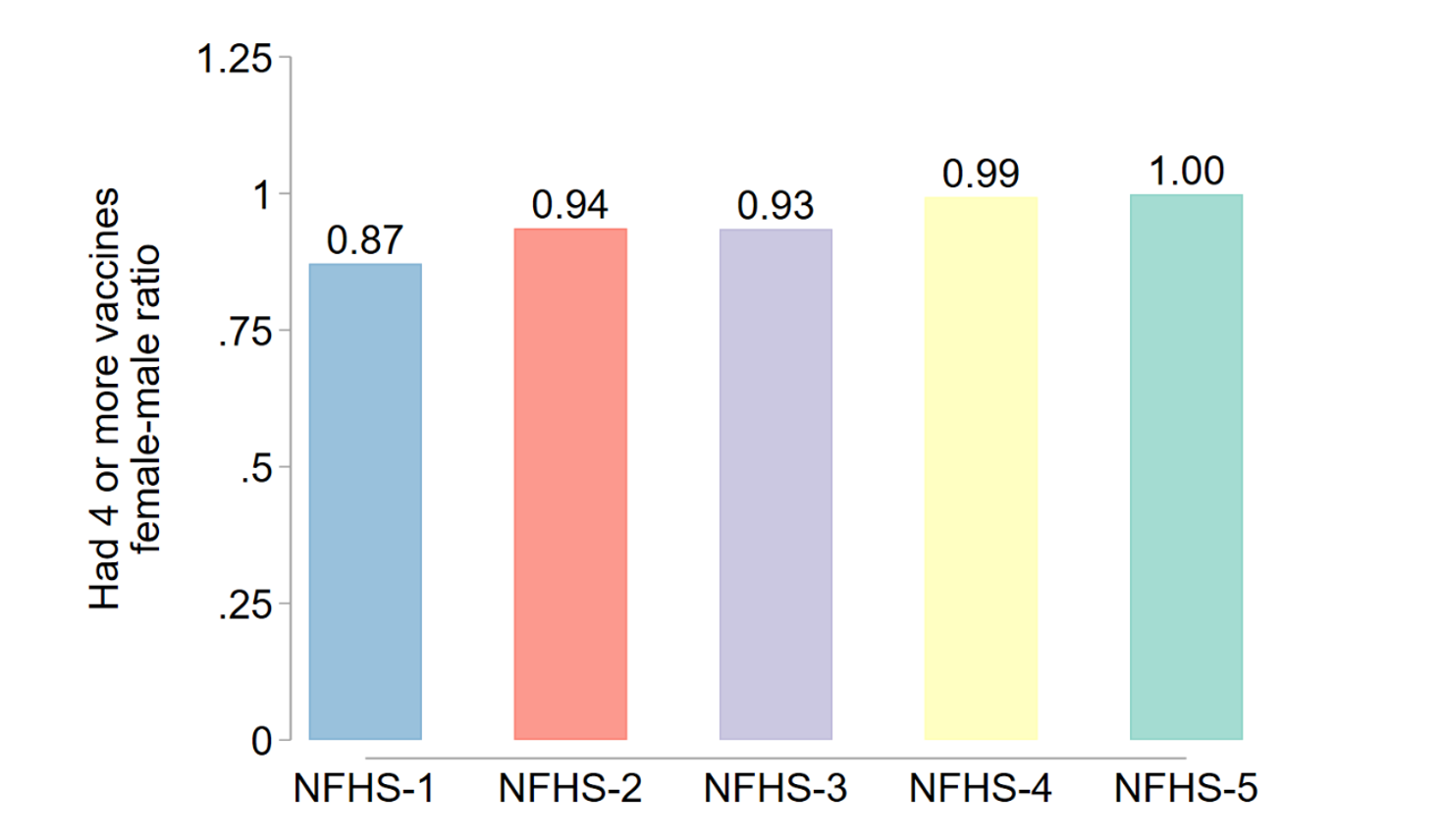
However, several studies document remaining gender gaps in health care. For example, Dupas and Jain (2023) analyse claims data from a health insurance programme in Rajasthan. Girls represent only 33% of hospital visits among children under 10 years old. This gender gap exists despite health care being free at public and private hospitals, which highlights the policy need to also compensate parents’ time and travel costs, for example by reimbursing travel costs or offering cash transfers conditioned on take-up of routine health care for girls.
Eldest son preference
Fact 4: There are stark health gaps between eldest sons, who are typically favoured, and other sons.
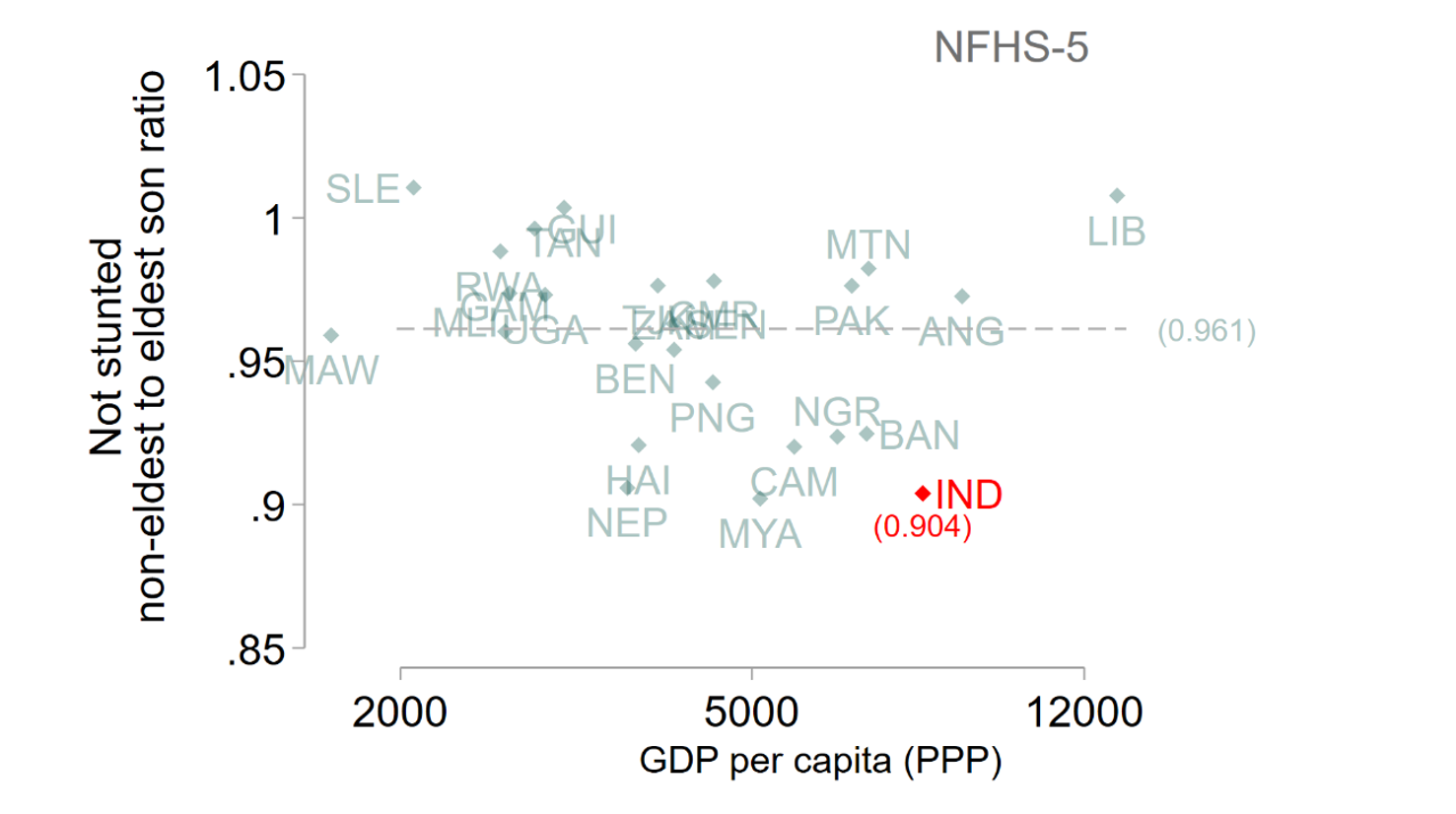
All sons are not treated equally. Eldest sons play special roles in the family such as providing old-age support for parents, and this causes parents to favour them more. Figure 2 plots the ratio of not being stunted (better health) for non-eldest sons compared to eldest sons. I compare India to other countries with Demographic and Health Surveys collected around the same time as NFHS-5. In comparison countries, the ratio is 0.96, on average; non-eldest sons fare somewhat worse than eldest sons worldwide. However, India is a negative outlier with a ratio of 0.90, signifying a stronger favouritism towards eldest sons.
Figure 2: Ratio of non-eldest to eldest sons’ absence of stunting (NFHS-5)
Facts 5 to 7: The desire to have at least one son – to play the eldest son role – drives the skewed sex ratio, which is not abating. The downward trend in family size is exacerbating how the desire for a son translates into sex selection.
The sex ratio in India is particularly male-skewed for last births in the family when the previous children are daughters (Jayachandran 2015). This pattern is consistent with a premium on having at least one son, with couples completing their fertility once they have a son and using sex-selection to obtain one. This speaks against a general aversion to having daughters (for example because of dowry expenses), which might lead to widespread sex-selection even for first births.
Figure 3 shows that the sex ratio of births has not become less male-skewed over the past 25 years. The analysis uses a retrospective panel constructed from respondents in the third to fifth NFHS waves.
Figure 3: Female-male sex ratio at birth based on NFHS data
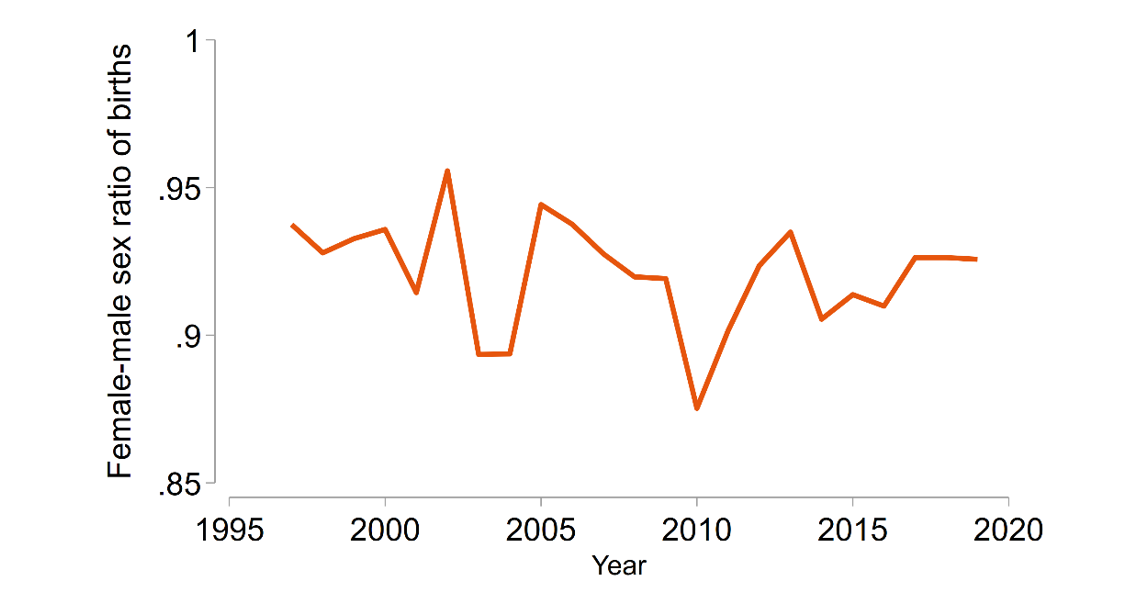
One factor that has impeded progress is the greater availability and affordability of sex determination technology. Another contributor is declining fertility. If parents want to have four children, the likelihood of ending up without a son is quite small, but if parents want just two children, a quarter of them will not have a son naturally so they are more likely to resort to sex-selective abortions to obtain a son.
Fact 8: Families’ quest for a son also has collateral damage on his sisters’ health.
An unintended consequence of parents’ quest for a son is that girls sometimes receive fewer inputs than boys. One channel for this is family size – a couple whose first two children are both sons, by chance, is more likely to stop having children than if the first two children are girls. The second couple will keep trying to have a son. This fertility behavior means that girls, on average, grow up in larger families, which have fewer resources to spend per child.
Jayachandran and Kuziemko (2011) show that because women in India are more likely to want to become pregnant again after a daughter is born, they stop breastfeeding girls sooner to regain their fecundity or because of the new pregnancy. Girls miss out on the health benefits of breastfeeding, even if parents do not explicit want to provide fewer health inputs to daughters.
Policy implications
Fact 9: Empowering women is not a panacea that will solve the problem of sex selection.
What policies can mitigate son preference and especially sex-selection? The fact that declining fertility exacerbates sex-selection upends some standard intuitions about policy solutions. A progressive policy such as educating girls so that they grow up to be empowered mothers might perversely worsen the sex ratio. This is because there are two offsetting effects: Education reduces son preference at any given family size, but it also decreases desired family size.
Table 1: Mother’s education does not decrease the desired sex ratio
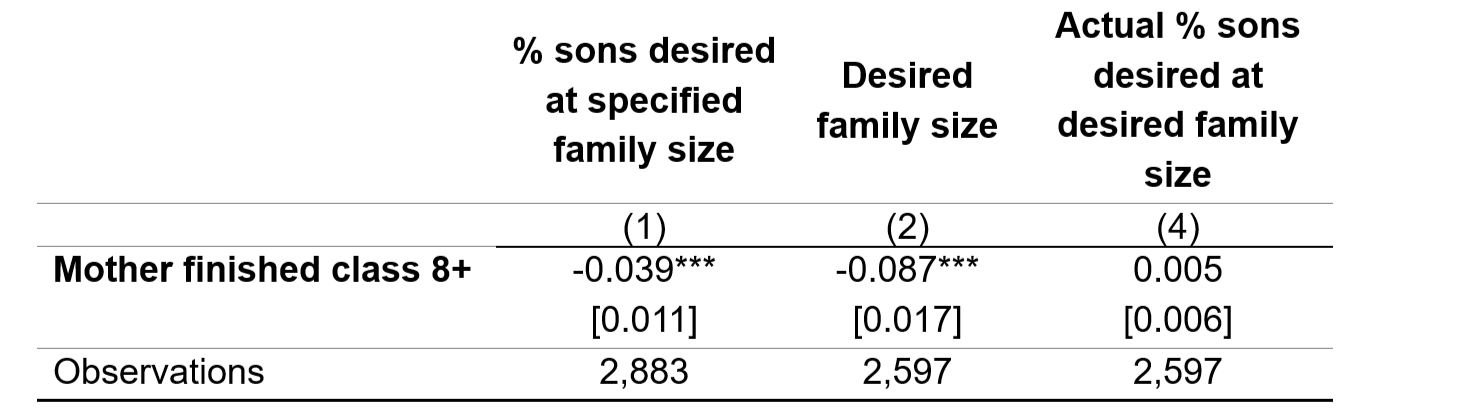
Notes: Standard errors, clustered by school, are in brackets. Asterisks denote significance: * p < :10, ** p < :05, *** p < :01. All regressions control for dummy variables for whether the father has completed primary school, grade 8, or grade 10+, and a cubic polynomial in the first principal component of several wealth variables. Data are from Jayachandran (2017).
Table 1 shows these offsetting forces, using data from Jayachandran (2017). Mothers were asked about the fertility outcomes they desired for their child. Column 1 shows that that mother’s education reduces the desired share of sons at a family size specified by the survey. This outcome measure captures their pure son preference, and education decreases it. Column 2 shows that education also leads to lower desired fertility. This uses the respondent’s response about the ideal family composition, encompassing both size and sex composition. Column 3 shows the net effect of these two offsetting effects. Female education does not improve the desired sex ratio (even if it has other benefits).
Fact 10: Offering financial incentives to have daughters risks further concentrating girls in poorer families.
One approach used to address the skewed sex ratio in India is financial incentives to have daughters. However, an extrinsic reward for having daughters risks crowding out the intrinsic value placed on them. Moreover, the policy could concentrate girls in poorer families because a given payment level will be more influential for fertility choices for a poor family than a rich one.
What policies, then, can work? This should be and is an active area of research and policy experimentation. Robust enforcement of the ban on sex-selection is important. Other policy options include ramping up delivery of health inputs and health care through schools, public pensions as an alternative to old-age support from sons, and policies that strengthen the intrinsic value that Indian families place on girls.
Editor's note: Another article covering this research can be found on IdeasforIndia.
References
Dupas, P, and R Jain (2023), “Women Left Behind: Gender Disparities in Utilization of Government Health Insurance in India,” Working Paper.
Jayachandran, S (2015), “The Roots of Gender Inequality in Developing Countries,” Annual Review of Economics, 7(1): 63–88.
Jayachandran, S (2017), “Fertility Decline and Missing Women,” American Economic Journal: Applied Economics, 9(1): 118–139.
Jayachandran, S, and I Kuziemko (2011), “Why Do Mothers Breastfeed Girls Less Than Boys? Evidence and Implications for Child Health in India,” Quarterly Journal of Economics, 126(3): 1485-1538.
Sen, A (1992), “Missing Women,” BMJ: British Medical Journal, 304(6827): 587.
Sen, A (1990), “More than 100 Million Women Are Missing,” New York Review of Books, 37.