





Where community interventions lead to behaviour change, continued interactions are needed to help people maintain healthy behaviours
Long-term continued adoption of welfare-improving goods and practices is fundamental to achieving the Sustainable Development Goals (SDGs). However, a drop in the adoption of such practices, and reversal to unsafe behaviour, is common after achieving initial improvements (Dupas and Miguel 2017). While promotion campaigns have, for example, proven effective at increasing learning and triggering behavioural change, how this change can be sustained over time is less well understood (Madajewicz et al. 2007, Duflo et al. 2015, Banerjee et al. 2015, Tarozzi et al. 2021, Chong et al. 2020, Hussam et al. 2021).
In a recent paper (Augsburg et al. 2022), we study the effectiveness of continued community-based mobilisation in rural Pakistan after the initial adoption of health infrastructure (household sanitation) was achieved. Using a randomised controlled trial, complemented by qualitative interviews, we find that without follow-up activities, the likelihood of reverting back to unsafe sanitation doubled in a two year period after the original intervention.
Conversely, positive effects on sustaining behaviour change lasted for at least one year after the implementation of follow-up activities. In addition, follow-up activities were significantly more effective where conditions to continue the improved behaviour were unfavourable, such as where toilets were initially in worse condition.
Beyond community-led total sanitation (CLTS) campaigns: Randomising follow-up activities
We leverage the recent completion of a community-led total sanitation (CLTS) campaign to study the effectiveness of continued activities in sustaining behaviour change. Implemented in more than 60 Latin American, Asian and African countries, CLTS is widely used to promote first-time adoption of private toilets. CLTS entails the delivery of health promotion and hygiene messaging through community meetings and other participatory activities.
We randomly allocated 61 villages, out of 123 villages in the Pakistani provinces of Sindh and Punjab where CLTS had been implemented, to receive follow-up activities. Follow-up activities were of two types:
- Broad-based community meetings (BBCMs) were held to assess general water, sanitation, and hygiene (WASH) status within the community, based on discussions promoted by local leaders and community walks. The aim of these gatherings was to review the progress on keeping the community ‘open-defecation-free’ as per the routine workplans, and to assign tasks designed during the Phase 1 CLTS campaign.
- Health and hygiene sessions (HHS), aimed at maintaining awareness regarding personal, domestic, and environmental hygiene conditions, were conducted door-to-door, as well as in community meetings. Besides delivering health and hygiene messages, the sessions also provided hand-washing demonstrations, and training on operation and maintenance of latrines.
As CLTS activities centre on promoting initial uptake rather than sustained change, the approach has been criticised for a lack of attention on slippage back to open defecation (OD).
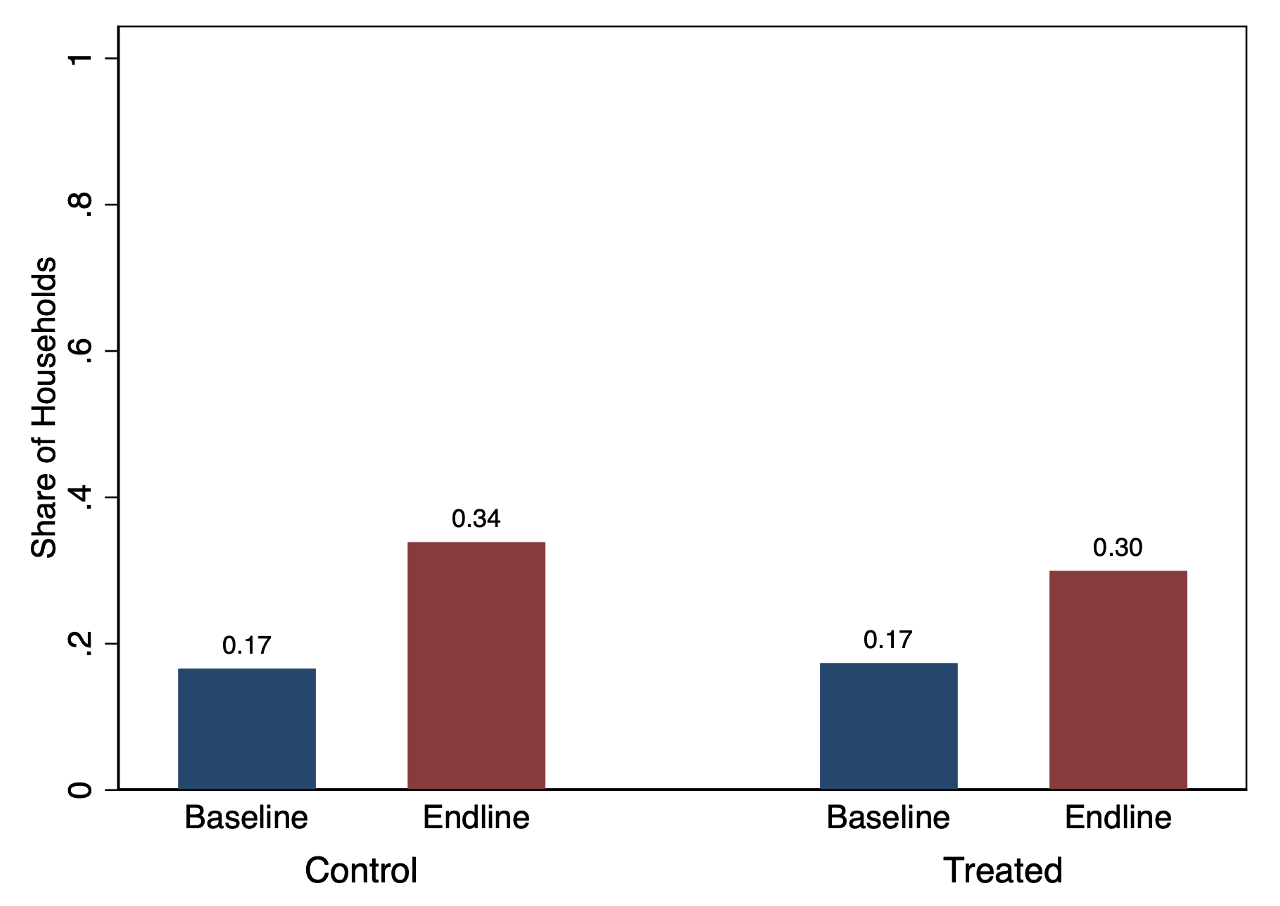
- As Panel A of Figure 1 (below) shows, among beneficiaries of the CLTS campaign, reversal to open defecation was common. Without follow-up activities, 34% of households in the control group (i.e. that did not live in areas where follow-up activities were implemented) reported OD practice two years post-CLTS completion, up from 17% after CTS completion.
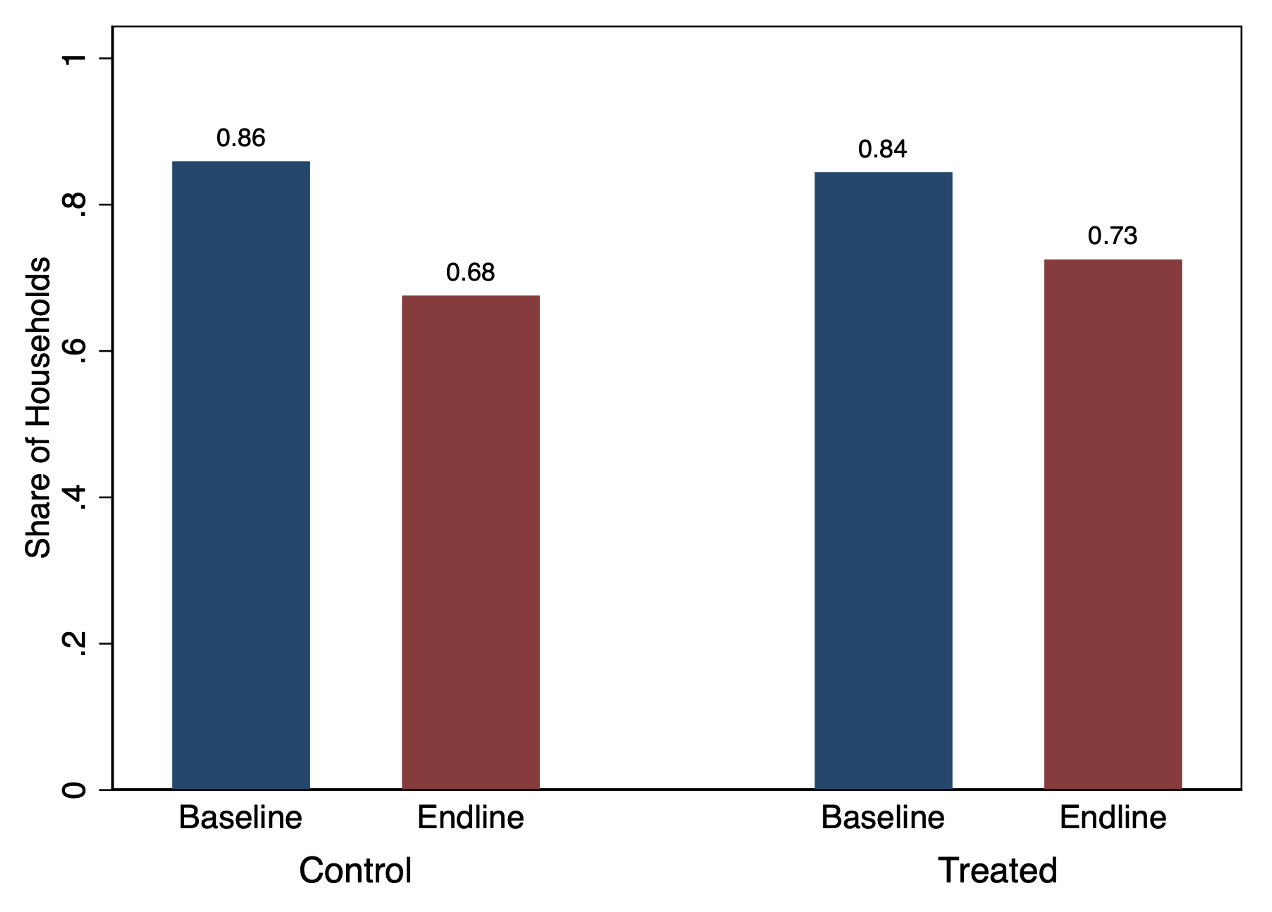
- In line with this, Panel B shows that only 68% of those in the control group reported using a functioning toilet at endline, down from 86% at baseline.
Figure 1 Reversal to unsafe sanitation and treatment effectiveness
A. Open defecation
B. Use functional latrine
Geographic variations in effectiveness of follow-up activities
Interviewing households that were exposed to a CLTS campaign initially, we find that `treated’ households (living in villages randomly allocated to receive follow-up activities) were 6 percentage points more likely to continue adopting safe sanitation behaviours. This effect is, however, only marginally significant, and how precisely it is estimated depends on the choice of specification.
We find, notably, that the effectiveness of the follow-up activities differed significantly by geographic location. Beneficiary households living in villages allocated to follow-up activities in the province of Sindh were, on average, 14 percentage points more likely to continue their improved sanitation behaviour, representing a 25% lower OD occurrence relative to control beneficiary households at endline. We find a comparably greater use of functional toilets in treated villages (13 percentage points higher), indicating that the lower OD was primarily due to sustained operability of the facilities.
Provinces differ not only in terms of the agency implementing the continued activities, but also in intervention-relevant characteristics. Sindh is a poorer province, with higher initial levels of OD, and where reversal to OD was the greatest among control households. As such, we investigate the sustainability of effects and heterogeneity in observed impacts focusing on the province of Sindh only.
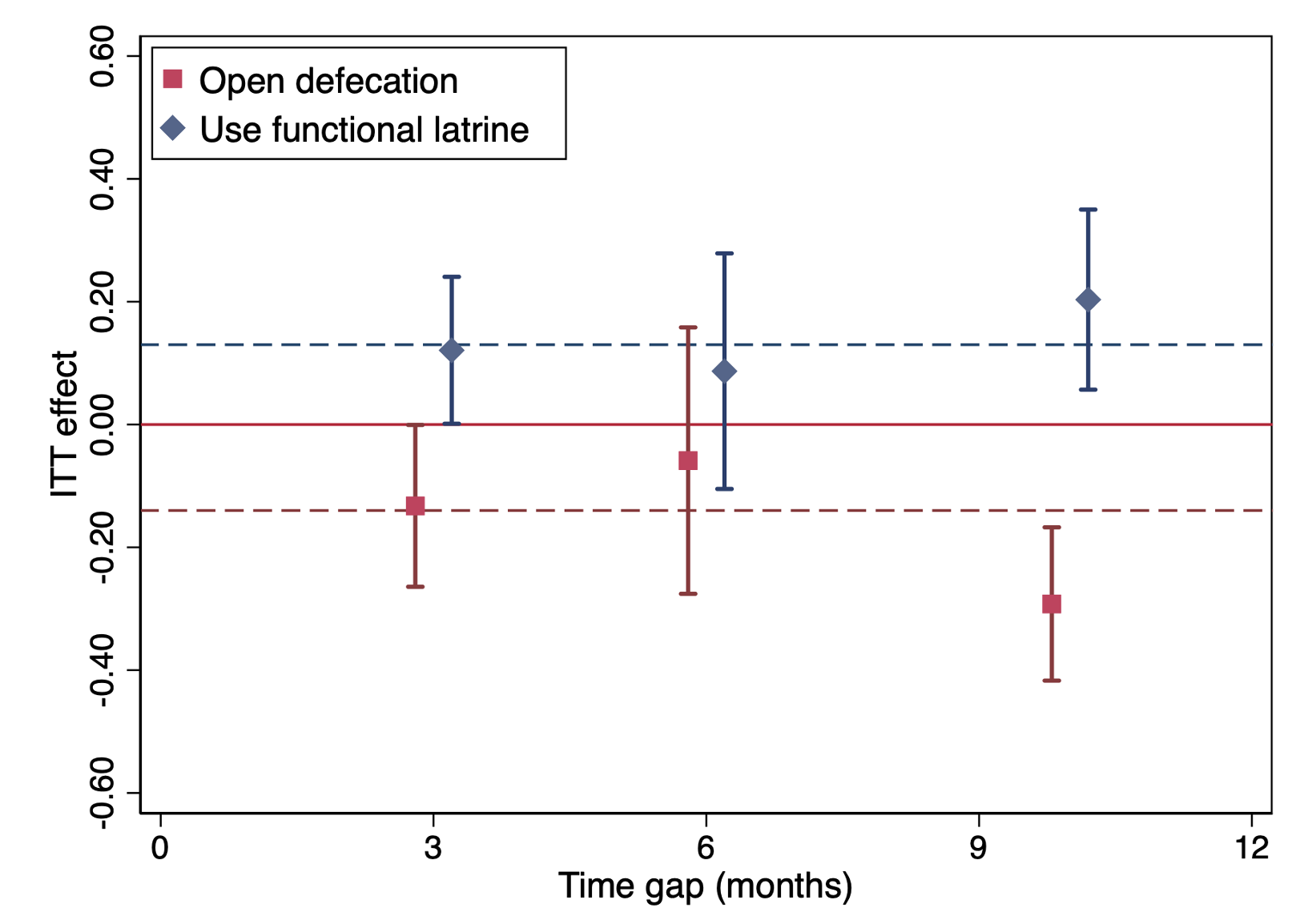
Figure 2 shows the estimated effects when splitting the treatment sample by time gap between follow-up activities and endline survey in Sindh. The results suggest that the reduction in OD due to follow-up activities is sustained over the first year. We also find some evidence to suggest that the average effects are even greater nine to twelve months after the intervention was finalised than they were three and six months after.
Figure 2 Effects of follow-up activities are sustained over time in Sindh
Targeting follow-up activities to minimise backsliding
Follow-up promotion efforts are best targeted towards those who are most likely to slip back into unsafe behaviour. We find that the material circumstances in which people initially live (including lack of access to public infrastructure and services, unfavourable environmental conditions of villages, asset poverty, and poor status of sanitation facilities) are all factors that affect the effectiveness of follow-up activities.
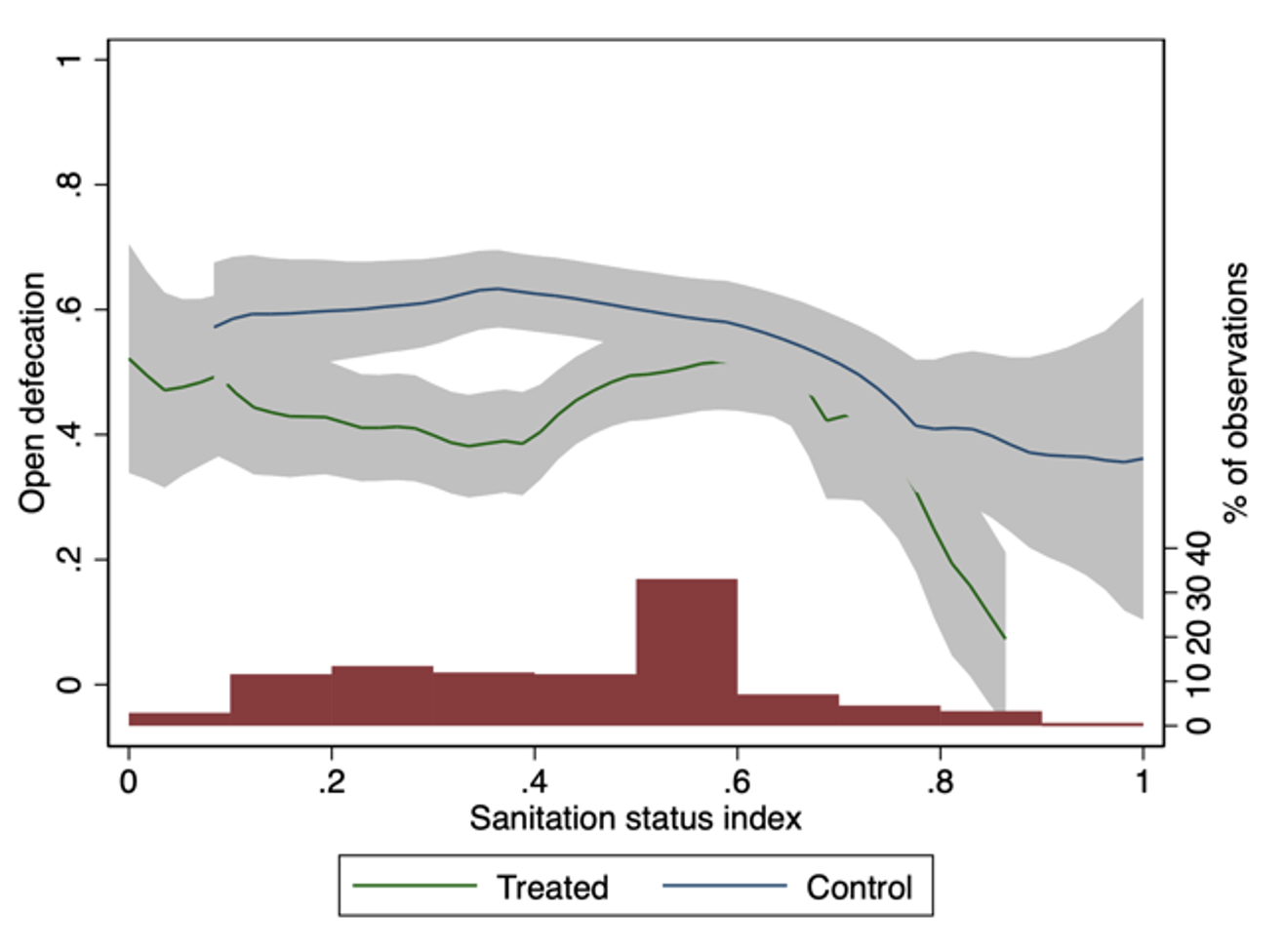
Follow-up activities are particularly effective in villages with poor public infrastructure (e.g. poor roads, which impede access to inputs for toilet maintenance). Beneficiary households in such villages are, on average, 28 percentage points less likely to revert to OD than treated households in villages with better initial public infrastructure. Likewise, beneficiary households allocated to follow-up activities in villages where sanitation and hygiene facilities were of poorer status at baseline were, on average, 16 percentage points less likely to practice OD than treated households with better sanitation facilities (see Figure 3).
We also find evidence to suggest that follow-up activities incentivised households living in these poor conditions to conduct regular maintenance of their latrines. These households also seem to have leveraged better latrine technologies and improved social norms to keep individuals away from harmful sanitation practices.
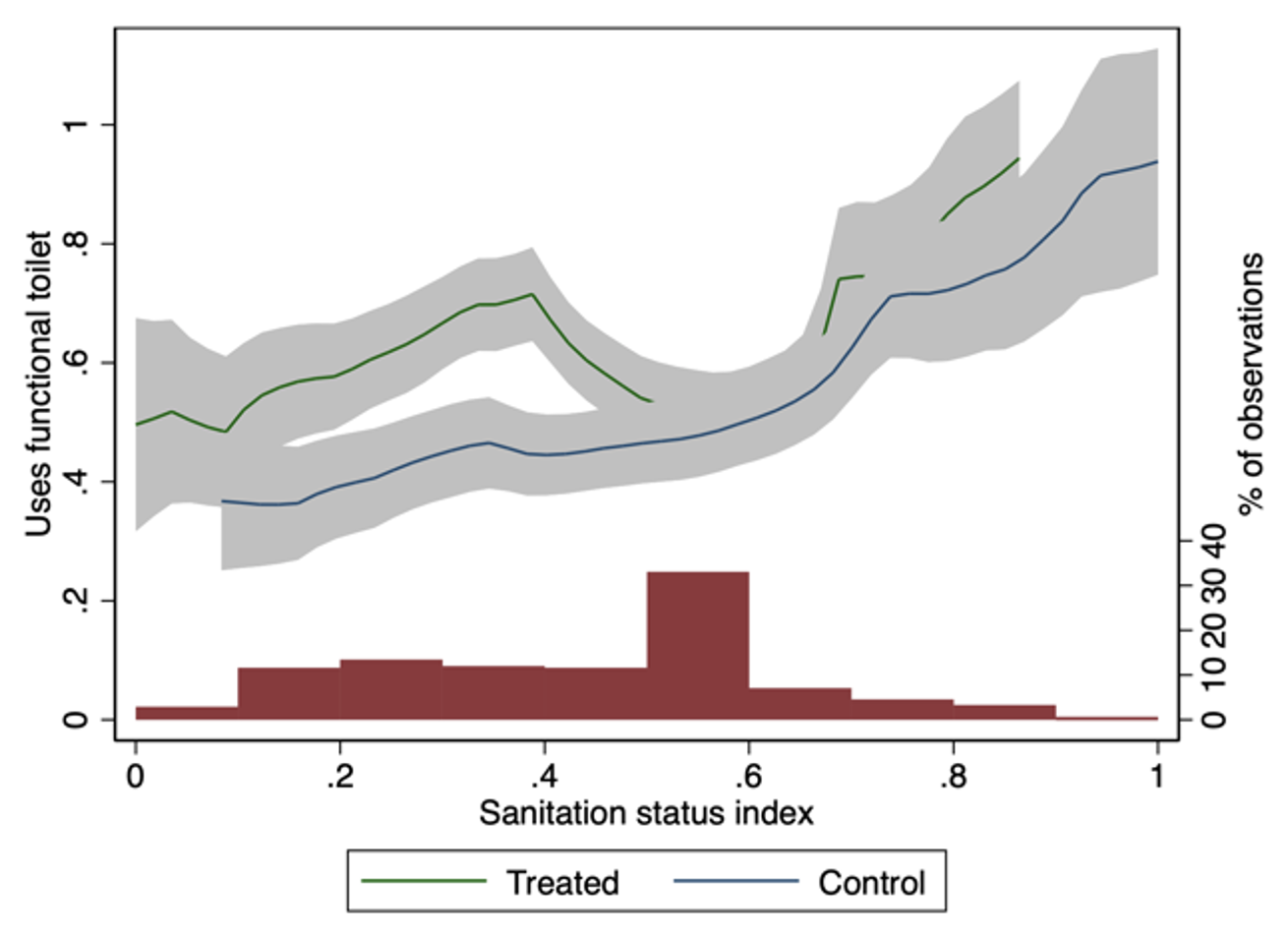
Figure 3 Greater effectiveness of follow-up activities when lower initial status of sanitation facilities in Sindh
A. Open defecation
B. Use functional latrine
Policy implications: Follow-up activities can increase cost-effectiveness of CLTS interventions
Our results stress that assumptions about post-intervention persistence in any CLTS cost- effectiveness analysis should adjust for slippage in behaviour; otherwise, the cost-effectiveness would be overstated. This is especially the case when CLTS was implemented in areas of poor public infrastructure. Furthermore, follow-up activities will likely improve the cost-effectiveness of CLTS.
Previous costing exercises of CLTS in several contexts reveal that the average CLTS programme cost is US$38 per targeted household (Crocker et al. 2017a). The impact of sanitation uptake, on the other hand, is estimated to lie between 4 and 23 percentage points on average (Patil et al. 2014, Guiteras et al. 2015, Pickering et al. 2015). Our estimated impacts of follow-up activities on using functional latrines at 6 percentage points on average and 13 percentage points in Sindh, do not fall short of these by much.
At the same time, the costs of follow-up activities are a small portion of overall program costs. Crocker et al. (2017b) highlight that training makes up a large portion of CLTS implementation costs (56%–61% of programme cost). The fact that this training has been completed by the time follow-up activities start makes it conceivable that the implementation of these activities is a worthwhile addition to the intervention as a whole.
References
Augsburg, B, A Bancalari, Z Durrani, M Vaidyanathan, and Z White (2022), “When nature calls back: Sustaining behavioural change in rural Pakistan”, Journal of Development Economics 158: 102933.
Banerjee, A, S Barnhardt, and E Duflo (2015), “Movies, Margins, and Marketing: Encouraging the Adoption of Iron-Fortified Salt”, in D Wise (ed.), Insights in the economics of aging, National Bureau of Economic Research.
Chong, A, M Gonzalez-Navarro, D Karlan, and MValdivia (2020), “Do information technologies improve teenagers’ sexual education? Evidence from a randomised evaluation in Colombia”, World Bank Economic Review 34(2): 371–392.
Crocker, J, D Saywell, K Shields, K, P Kolsky, and J Bartram (2017a), “The true costs of participatory sanitation: Evidence from community-led total sanitation studies in Ghana and Ethiopia”, Science of the Total Environment 601–602: 1075–1083.
Crocker, J, D Saywell, and J Bartram (2017b), “Sustainability of community-led total sanitation outcomes: Evidence from Ethiopia and Ghana”, International Journal of Hygiene and Environmental Health 220: 551–557.
Duflo, E, P Dupas, P, and M Kremer (2015), “Education, HIV, and early fertility: Experimental evidence from Kenya”, American Economic Review 105(9): 2757–2797.
Dupas, P and E Miguel (2017), “Impacts and determinants of health levels in low- income countries”, in A Banerjee and E Duflo (eds), Handbook of Economic Field Experiments, Vol. 2, Elsevier B.V., pp. 3–73.
Guiteras, R, J Levinsohn, and A.M. Mobarak (2015), “Encouraging sanitation investment in the developing world: A cluster-randomised trial”, Science 348(6237): 903–906.
Hussam, R, A Rabbani, G Reggiani, and N Rigol (2021), “Rational habit formation: Experimental evidence from handwashing in India”, American Journal of Applied Economics 14: 1–41.
Madajewicz, M, A Pfaff, A van Geen, J Graziano, I Hussein, H Momotaj, R Sylvi, and H Ahsan (2007), “Can information alone change behaviour? Response to arsenic contamination of groundwater in Bangladesh”, Journal of Development Economics 84(2): 731–754.
Patil, S, B Arnold, A Salvatore, B Briceno, S Ganguly, J Colford, and P Gertler (2014), “The effect of India’s total sanitation campaign on defecation behaviours and child health in rural Madhya Pradesh: A cluster randomised controlled trial”, PLoS Med. 11 (8): e1001709.
Pickering, A, H Djebbari, C Lopez, M Coulibaly, and M Alzua (2015), “Effect of a community-led sanitation intervention on child diarrhoea and child growth in rural Mali: A cluster-randomised controlled trial”, Lancet Global Health 3(11): e701–e711.
Tarozzi, A, R Maertens, K Matin Ahmed, and A van Geen (2021), “Demand for information on environmental health risk, mode of delivery, and behavioural change: Evidence from Sonargaon, Bangladesh”, World Bank Economic Review 35: 764–792.