





Privatising sludge treatment centres improves sanitation outcomes and reduces desludging prices without concentrating market power
Poor management of public utilities in developing countries can contribute to low public welfare. Governments in developing countries often lack the managerial capacity and budget to maintain the substantial capital equipment required to effectively run utilities, and the government’s political objectives may hinder the successful operation of the utility (Galiani 2021). Inefficiencies may compound when the government manages an upstream industry, as the effects of poor management reverberate throughout the sector. Yet, the privatisation of public utilities can also reduce efficiency, providing opportunities for companies to vertically integrate and generate market power.
Much of the evidence on privatisation from Eastern Europe and Latin America suggests that there are potentially large improvements from privatisation across a variety of sectors (Barberis et al. 1996, Megginson and Netter 2001, Galiani et al. 2005). However, there is little evidence in Africa where the welfare impacts of privatisation may be much larger (Kosec 2014). In 2013, Senegal’s government privatised the management of one piece of Dakar’s sanitation sector: sludge treatment centres. In our recent paper (Deutschmann, Gars, Houde, Lipscomb and Schechter 2021) we measure the impact of this privatisation on downstream sludge-removal businesses and on public welfare.
Privatising sludge treatment centres
Sludge treatment centres are a key component of the sanitation business. As of 2013, about three quarters of households in Dakar were not connected to the sewage system (Sene 2017), and most of these households have toilets which empty into pits that fill up every 6-12 months. They may then hire a trucker to desludge (empty) the pit, after which the trucker dumps the sludge at a treatment centre before continuing to his next job. Poor management of treatment centres has important repercussions: insufficient operating hours at treatment centres (either due to centres being closed on weekends, having short weekday hours, or being closed for repairs) and delays due to slow lines will reduce the number of jobs that a trucker can do in a day. High costs of dumping at treatment centres may induce truckers to pass on the costs to households, or to illegally dump in public waterways or open spaces rather than at treatment centres. This may result in high prices, unsanitary illegal dumping, and low numbers of jobs being completed, which impose health costs as households switch to inferior (manual) services in which the sludge is disposed of in streets near the house.
Privatisation can directly increase the productivity of treatment centres, and thus indirectly increase the productivity of desludging truckers. However, privatisation is not necessarily a panacea for the problems of the sanitation sector. Privatised management of the treatment centres could lead to market power, particularly if the treatment centres are managed by actors from the downstream trucking market. This could lead to lower quantities of services provided and welfare transfers from consumers to a few connected suppliers.
Effects of privatising Dakar’s sanitation treatment centres
The case of sanitation treatment centres in Dakar provides an excellent case study for privatisation. In 2013, Dakar’s sludge treatment centres were poorly managed and in disrepair. Centres were open for short business hours and often experienced mechanical issues as they operated substantially beyond their designed processing capacity, forcing them to stop operations for weeks at a time. Desludging truck operators and their Association (AAAS) resorted to helping with the maintenance to keep the centres operational. Given the difficulties in managing the treatment centres, the government decided to privatise them. In November 2013, management responsibility was delegated to Delvic Sanitation Limited, a new venture run by the combined Delta and Vicas trucking companies – two of the largest sanitation truck operators in the city. Delvic was tasked with operating the government-owned treatment centres and was allowed to keep 50% of the revenue from dumping payments after paying the government a leasing fee.
We collected the universe of all sludge dumped at Dakar treatment centres from May 2009 to October 2018, including information on the truck’s license plate, the company, and the date. Using this data, we measure the change in the amount of sludge dumped at treatment centres, and the market share of desludgings by the two trucking companies managing the treatment centres. In addition, we use household survey data to measure impacts on desludging prices, the choice between manual and mechanical desludging, and child diarrhoea outcomes.
We show that privatisation increased the amount of legal dumping at the treatment centres by 64%, and led desludging trucks to complete more jobs per day. We do not find evidence of market capture by the two firms managing the treatment centres. The implied decrease in cost for truck drivers was 7% of the cost of a desludging job.
Much of this cost decrease was passed through to the households — privatisation reduced prices for households by approximately 4.6% and led to a 2.4 percentage point increase in the probability that a household would choose to use mechanical desludging when their latrine pit was full. Given the relatively small increase in demand, our results suggest the large increase in sludge dumped at the treatment centres was primarily caused by a decrease in illegal dumping by the trucks. The improved disposal of sludge—through reductions in both illegal dumping and manual desludging – led to important health benefits. Privatisation was associated with a 22 percentage point decline in child diarrhoea in Dakar relative to other areas of Senegal.
The impact of privatisation on the desludging business
Figure 1 Total volume of sludge treated at centres
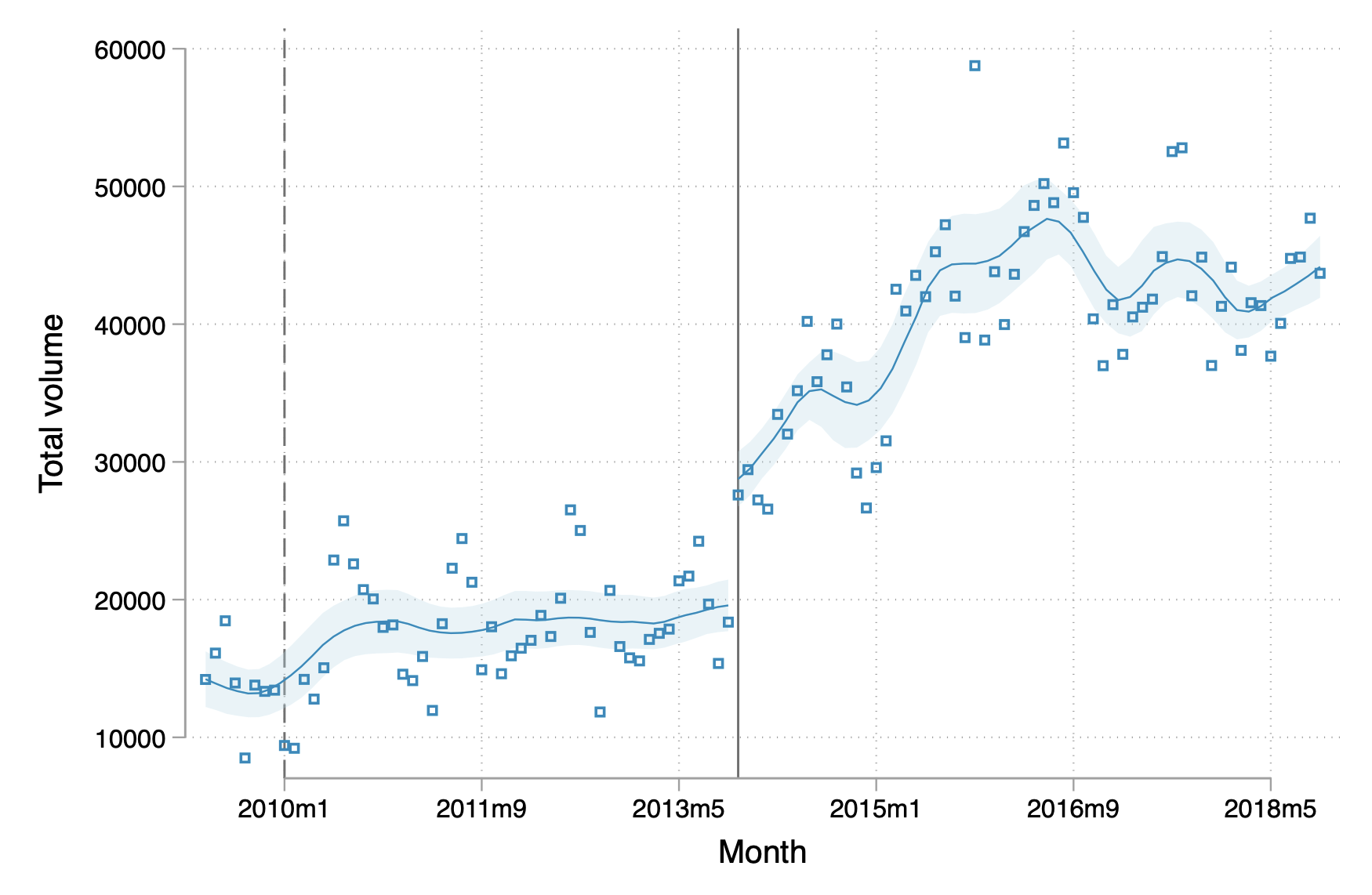
Note: The figure shows the volume of sludge treated by centres between May 2009 and November 2018, with a vertical line marking the time of privatisation.
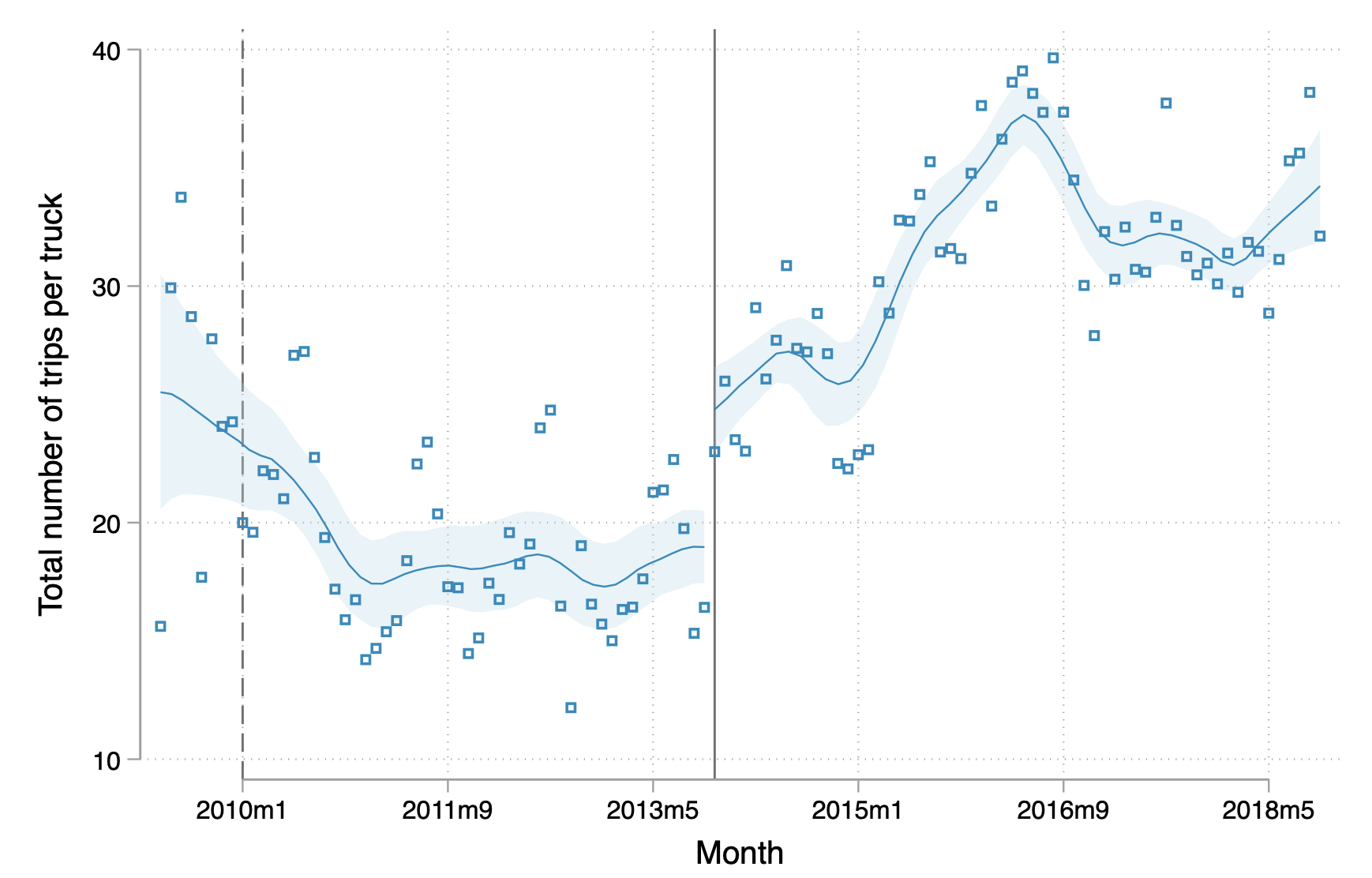
There was a large increase in the volume of treated sludge at the treatment centres immediately following privatisation, corresponding to both an increase in the number of trucks using the centre each month and an increase in the number of completed trips. Increased volume at the centres came from all sanitation companies, not just the two that managed the privatised treatment centre. This suggests that privatisation did not increase the market power of those companies. Figure 1 shows that treated volume had been steady prior to privatisation but made a sudden jump and then continued to grow following privatisation. Overall, we find a 64% increase in volume following privatisation.
We show that this increase in volume occurs both for the two companies managing the centres and in the rest of the market. The companies managing the centres were unsuccessful at exerting market power after vertically integrating. Government regulation fixing the price of dumping at the treatment centres may have made it more difficult to extract rents or foreclose competitors. Increased volume derives primarily from increased capacity utilisation of the trucks that were already on the road rather than from a large influx of new trucks in the market. In part, this is linked to an expansion in the number of hours the treatment stations are open as traffic at the treatment centres increased on weekends and later in the day on weekdays.
The impact of privatisation on household welfare
Figure 2 Incidence of diarrhoea amongst children under 5 in Dakar vs other urban areas in Senegal
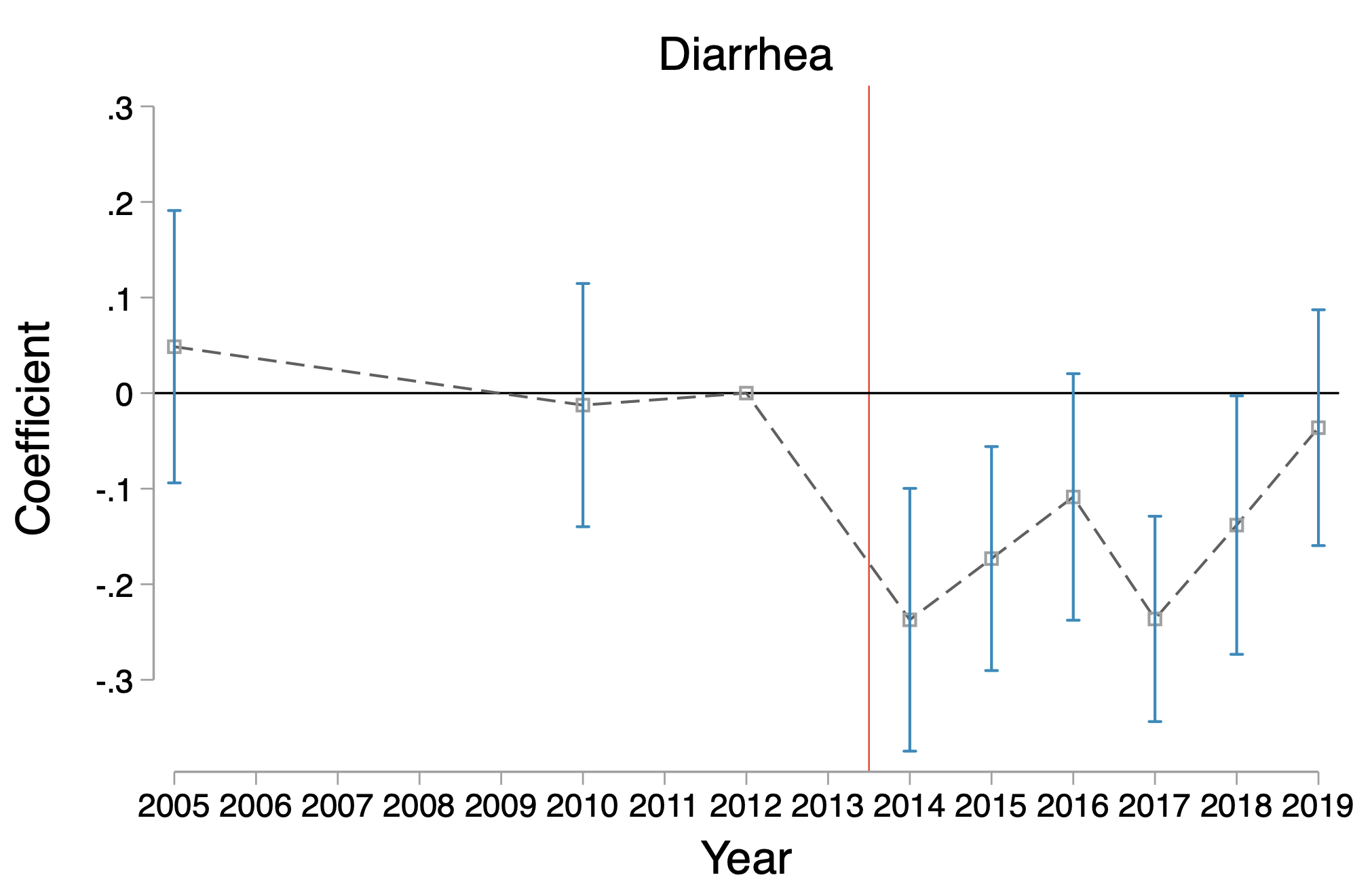
Note: The figure plots the coefficients from running an event study regression where the dependent variable is the incidence of diarrhoea. The omitted category is 2012, the year leading up to the 2013 privatisation (signified with the red line).
The reduction in input costs generated by the privatisation led to reduced prices for consumers, some evidence of higher take-up of more sanitary mechanised desludgings, and improved health. We use a retrospective household survey of sanitation use of 4,331 households to evaluate the impact of the privatisation on whether the household purchases a mechanised desludging when they need to empty their latrine (rather than manual desludging, which is cheaper but less sanitary) and on the price of the mechanised desludging. We find that prices decrease by 1,071 CFA on average, which represents a 4.6% decrease at the mean of 23,357 CFA. This corresponded with a 2.4 percentage point increase in the use of mechanised desludging.
We also test the impact of the reform on local health by comparing diarrhoea rates in Dakar over time to diarrhoea rates outside of Dakar. We find that privatisation led to a 22 percentage point decline in diarrhoea incidence relative to other urban areas of Senegal. As shown in Figure 2, diarrhoea rates were relatively similar to other urban areas of Senegal prior to privatisation, but quickly decreased in Dakar following privatisation, while remaining steady in regional cities. A similar impact is not found in the incidence of cough, a symptom that we would not expect to be directly related to sanitation-related illnesses.
Policy implications and caveats
We show that there is a large increase in volume at sanitation treatment centres following privatisation. This corresponds with a decrease in the mechanised desludging price paid by households, an increase in the use of mechanised desludging, and a decrease in diarrhoea rates relative to other urban areas of Dakar.
It is important to note that unlike a full privatisation, the management of the centres was delegated to a private company. The private company did not own the capital, and was only licensed to operate the centres for a few years. The private company was also constrained by regulations to maintain the prices it charged for services. Privatisation under different contractual arrangements could yield substantially different results.
One concern about privatisation of a component of the utility supply chain would be if it were to create market power. We show that this instance of privatisation did not lead to an increase in market power by the companies managing the privatised treatment centres. Rather, there was an increase in the productivity of trucks owned by all companies in the sector.
References
Barberis, N, M Boycko, A Shleifer and N Tsukanova (1996), “How does privatization work? Evidence from the Russian shops”, Journal of Political Economy 104(4): 764-790.
Deutschmann, J W, J E Gars, J F Houde, M Lipscomb and L Schechter, L (2021), “Privatization of public goods: Evidence from the sanitation sector in Senegal”, NBER Working Paper 29295.
Galiani, S (2021), “Public Sector Participation in the Water Sector: Opportunities and pitfalls”.
Galiani, S, P Gertler, and E Schargrodsky, E (2005), “Water for life: The impact of the privatization of water services on child mortality”, Journal of Political Economy 113(1): 83-120.
Kosec, K (2014), “The child health implications of privatizing Africa's urban water supply”, Journal of Health Economics 35: 1-19.
Megginson, W and J M Netter (2001), “From state to market: A survey of empirical studies of privatization”, Journal of Economic Literature 39(2): 321-389.
Sene, M (2017), Increasing financial flows for urban sanitation: Case study in Dakar, Senegal, Technical report, World Water Council.